Congenital microtia is a congenital condition characterized by abnormal development of the outer ear, with clinical manifestations ranging from “slightly smaller ear with basic structure intact” to “complete absence of the ear”.
Due to the complex morphology of the deformity, various classification methods have emerged internationally. However, the core significance of classification in clinical treatment lies in guiding different patients to choose appropriate treatment plans.
The Ear Reconstruction Team at the Chinese Academy of Medical Sciences Plastic Surgery Hospital has classified congenital microtia into four major categories based on over a decade of clinical experience with tens of thousands of ear reconstruction cases: Type I, Type II, Type III, and Type IV.
This classification is more aligned with surgical decision-making and provides a clearer understanding of treatment pathways for patients and their families. Below, I will detail this classification method. If you can read Chinese papers, feel free to message me for the original paper.
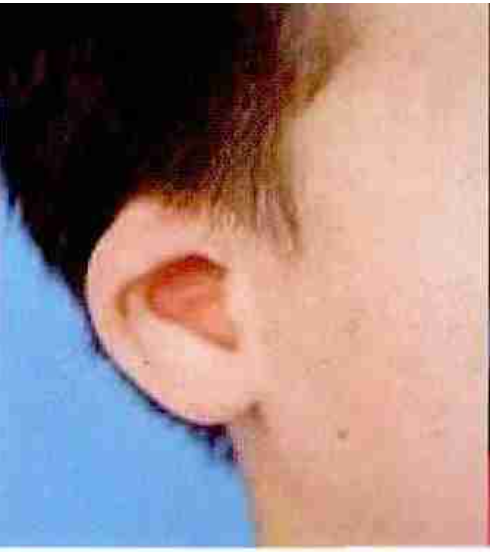
Type I Microtia: Basic Structure Intact, Only Smaller in Size

Main Characteristics:
- The main anatomical structures of the ear (auricle, antihelix, earlobe, external auditory canal, etc.) are basically present.
- The overall contour of the ear is relatively small.
- Often associated with mild ear deformities such as cup ear and protruding ear.
- Visually recognizable as “an ear”.
Clinical Significance:
Type I is not strictly a “deficient microtia” and usually does not require auricular reconstruction surgery. Treatment goals include:
- Adjusting the size difference between both ears.
- Correcting morphological issues such as cup ear and protruding ear.
- Improving symmetry through local correction or composite tissue transplantation.
Type II Microtia: Partially Recognizable Structures (Divided into IIA and IIB)
Type II is a category that lies between “mild deformity” and “severe deficiency”, where some ear structures are still identifiable, but overall development is significantly insufficient.
Type IIA: Relatively More Cartilage, Can Partially “Expand and Shape”
Performance Characteristics:
- Significant folding of cartilage in the upper part of the auricle.
- Although the structure is incomplete, there is a relatively large amount of folded cartilage.
- The transverse width of the auricle is relatively acceptable.
Treatment Approach:
- Conservative treatment: Use an external corrective device within 2-3 months after birth.
- Surgical shaping: If conditions permit, perform cartilage expansion surgery at 1.5-2 years to release growth potential.
- Composite tissue transplantation: Recommended after school age (when auricular development has basically stopped).
Type IIB: Insufficient Cartilage, Requires Auricular Reconstruction

Performance Characteristics:
- Little cartilage in the upper part of the auricle.
- Even if the folds are released, it is difficult to restore the basic shape.
- Overall size of the auricle is significantly insufficient.
Treatment Approach:
- Usually requires standard auricular reconstruction.
- Reshape the auricle using rib cartilage scaffolding or other reconstruction methods.
Type III Microtia: Most Common Type, Structure Difficult to Recognize

Main Characteristics:
- The anatomical structure of the auricle is basically unrecognizable.
- The residual ear often presents irregular appearances such as “peanut-shaped, sausage-shaped, or cord-like”.
- Most cases are accompanied by external auditory canal atresia or absence of the ear canal.
Clinical Significance:
This is the most common type of microtia encountered clinically. Treatment primarily focuses on auricular reconstruction, with key points including:
- Fully utilizing residual ear tissue.
- Reconstructing a complete auricle using autologous rib cartilage or expanded flaps.
- Emphasizing the three-dimensional structure and positional symmetry of the auricle.
Type IV Microtia: Severe or Complete Absence of Ear Deformity

Main Characteristics:
- The affected side has only a very small skin tag or scattered protrusions.
- Or there is a complete absence of any auricular remnants.
- There is almost no usable residual ear tissue locally.
Clinical Significance:
Type IV is the most severe type, requiring “total ear reconstruction”:
- Complete reconstruction of the outer ear, including the earlobe.
- High surgical complexity, with greater demands on skin, cartilage scaffolding, and blood supply conditions.
- The reconstruction outcome is closely related to the choice of surgical technique and the surgeon’s experience.
Why is Classification Important?
Different types of microtia vary greatly in surgical strategy, timing, difficulty, and expected outcomes:
- Type I: Primarily corrective, does not involve complete ear reconstruction.
- Type II: Some can be managed with “preservation + reshaping”, while some require reconstruction.
- Type III: The main population for standard auricular reconstruction.
- Type IV: Complete outer ear reconstruction, with the highest surgical difficulty.
Therefore, accurate classification is the first step in developing a treatment plan and is an important prerequisite for the success of the surgery.
Information Source
Classification and Treatment Strategies for Congenital Microtia (Authors: Jiang Haiyue, Pan Bo, Lin Lin)