Congenital microtia is one of the most severe physiological defects in the development of the outer ear. Currently, the use of autologous rib cartilage for auricular reconstruction is recognized as the international mainstream surgical method for treating this condition, with the core principle being to utilize the patient’s own cartilage to construct a complex three-dimensional ‘ear framework’.
Timing of Surgery and Developmental Requirements
Although the auricle reaches 95% of its adult size by age 6, the volume and hardness of the rib cartilage are the physical foundations for the success of the surgery. The minimum standards recommended by clinical consensus are:
- Age Requirement: The child must be at least 6 years old.
- Developmental Indicators: Height must be greater than 120 cm, and the chest circumference below the xiphoid process must be greater than 60 cm.
- Special Cases: For adult patients with significant calcification of rib cartilage, preoperative imaging assessment of cartilage quality is necessary to determine the most suitable carving plan.
Cartilage Carving
Autologous rib cartilage reconstruction typically requires harvesting the 6th, 7th, and 8th rib cartilages. Each piece of cartilage plays an irreplaceable role in the ‘new ear’:
- Base Plate (6th and 7th Ribs): Forms the main body of the framework, simulating the depth of the concha and triangular fossa.
- Auricular Rim (8th Rib): Due to its elongated shape, it is often used to carve a rounded, smooth auricular rim and antihelix.
- Splicing and Fixation: Remaining cartilage fragments will be used to reinforce the framework or carved into the antihelix and contralateral antihelix. All cartilage components must be precisely spliced using titanium wire of about 0.2 mm, with all knots placed on the back to prevent skin perforation.
Surgical Steps: Phased Reconstruction
Phase One: Framework Placement and Earlobe Positioning
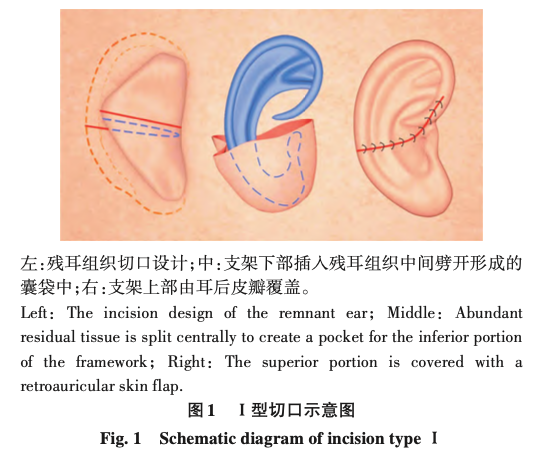
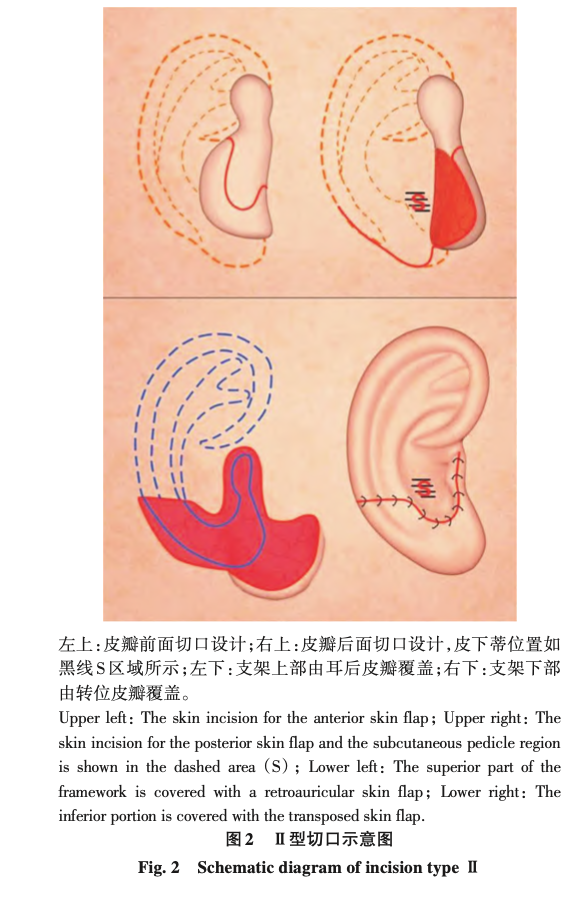
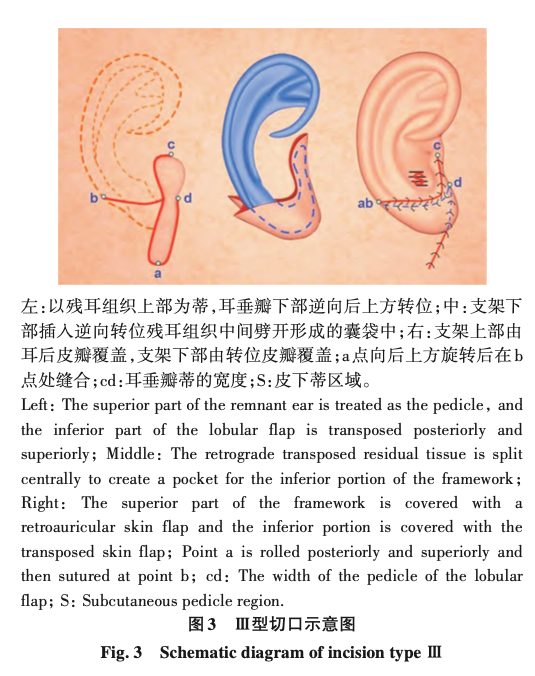
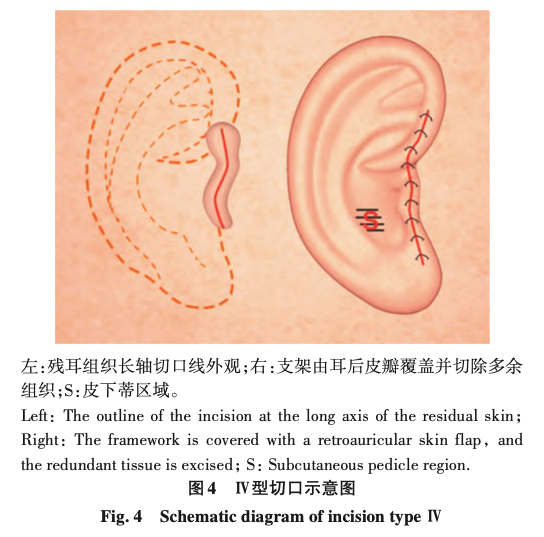
- Incision Design: Design a personalized surgical incision based on the amount of residual ear tissue (e.g., sausage-type, concha-type, etc.).
- Pocket Preparation: Remove the twisted cartilage within the residual ear and dissect a flap pocket that can fully accommodate the framework.
- Framework Insertion: Precisely insert the carved rib cartilage framework and adjust the earlobe position to maintain proportionality with the face.
Phase Two: Reconstruction of the Craniomandibular Angle (Otoplasty)
- Timing of Surgery: Usually performed 3-6 months after the first stage.
- Angle Reshaping: The goal is to make the ‘ear’ that is ‘stuck’ to the head ‘stand up’. The surgeon will lift the framework and embed a small C-shaped cartilage framework (or artificial material) on the back as support.
- Covering with Skin Graft: Use a postauricular fascial flap to cover the supporting material, followed by skin grafting to form a natural three-dimensional structure of the craniomandibular angle.
Postoperative Care and Potential Complications
Due to the non-regenerative nature of rib cartilage and limited skin capacity, long-term protection after surgery is crucial.
| Complication Type | Prevention and Core Management Strategies |
|---|---|
| Thoracic Deformity | Strictly adhere to the surgical age threshold, and preserve the perichondrium as much as possible during surgery to promote cartilage regeneration. |
| Flap Necrosis/Cartilage Exposure | The edges of the framework must be rounded and smooth; postoperative adjustment of negative pressure drainage, and high-pressure oxygen therapy if necessary. |
| Framework Deformation | Avoid impact and pressure within 3 months post-surgery, sleep on the non-affected side, and wear a custom postauricular framework long-term. |
| Infection | Strict aseptic techniques and disinfection of the external auditory canal; if redness, swelling, or exudation occurs, timely debridement and drainage are necessary. |
Information Source
Expert Consensus on the Application of Autologous Rib Cartilage for Total Ear Reconstruction in Congenital Microtia (2025)